The number of poliomyelitis (polio) cases outside the three endemic countries (Nigeria, Pakistan and Afghanistan) increased in 2013 compared to 2012, including a recent outbreak in war-torn Syria. Israel has not seen any paralytic infections but has found evidence of the disease in environmental samples at 25 separate sites.
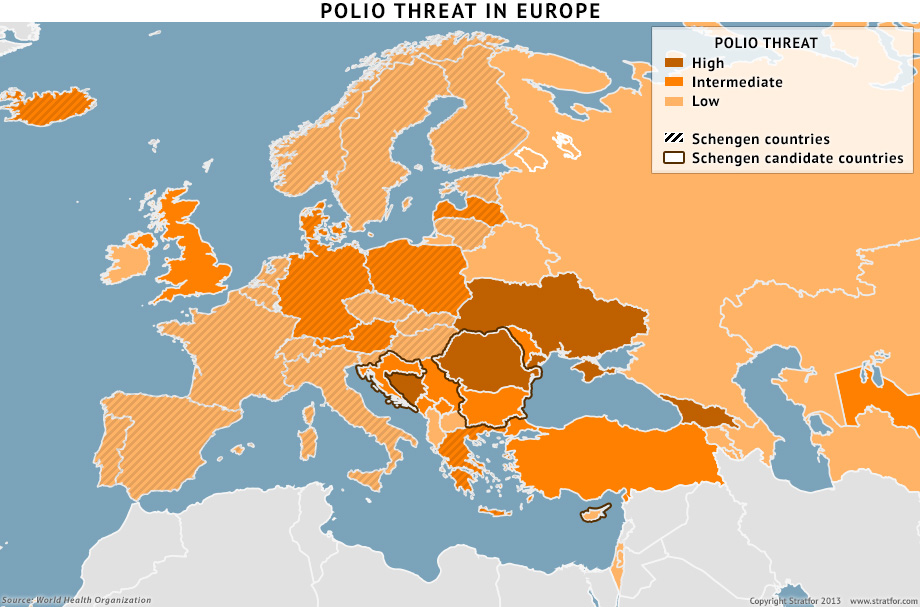
Given the proximity of the outbreak in Syria and the influx of asylum seekers from the Middle East, several European countries face a heightened risk of polio infections within their borders. The free movement of people across the borders of EU countries that are part of the Schengen Agreement — regarded as a symbol of the European project's success — could be limited in the future. This is especially true for Eastern European countries seeking to enter the Schengen zone, since border security has already been questioned. Even before this re-emergence of polio in the Middle East, there was widespread opposition to Romania and Bulgaria joining the Schengen zone. Negative publicity regarding a potential outbreak of infections such as polio could contribute to the rising skepticism about deeper European integration.
Polio does not have a lasting impact on a large portion of the population. In 1988, before the disease was widely eradicated globally, there were 350,000 cases of polio-associated paralysis. In fact, most people infected with the virus are asymptomatic; only one in 200 infected individuals will experience paralysis. However, the disease targets children, and the lasting effects of paralysis on a child give the disease a disproportionally large psychological impact.
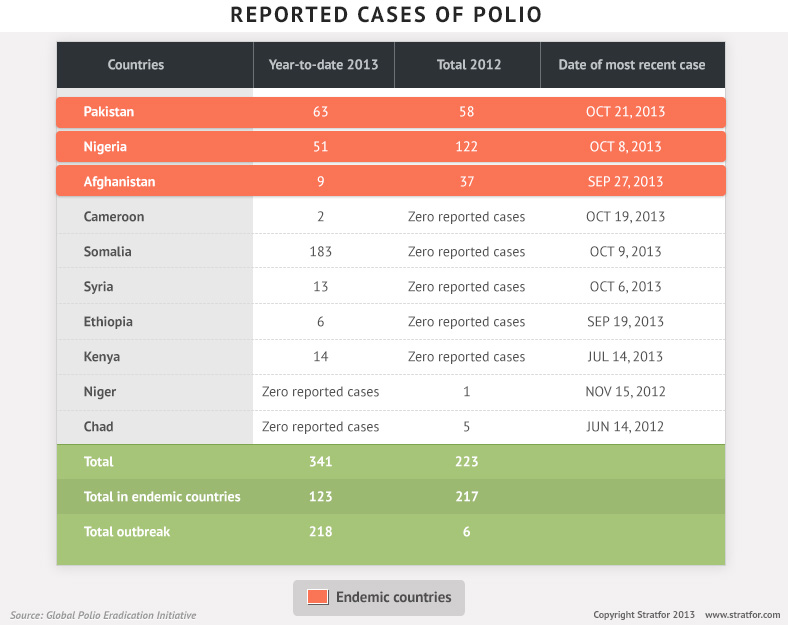
Polio cases around the world decreased from 1,652 reported cases in 2008 to only 223 reported cases in 2012. Almost all of the cases in 2012 occurred in Afghanistan, Pakistan and Nigeria, where the disease remains endemic. However, reported infections in 2013 have already reached 341, with 218 cases occurring in non-endemic countries. The largest concentration of these infections has been in Somalia, where the risk of reoccurrence is high due to low immunization rates (caused by instability in the country, poor infrastructure and al Shabaab's movement against vaccinations) and its geographic proximity to Africa's poliovirus importation belt, which stretches from Nigeria to the Horn of Africa.
Outside eastern Africa, the highest number of infections for non-endemic countries occurred in Syria, with 13 confirmed cases and more cases suspected. The source of the Syrian outbreak has been traced back to Pakistan. Immunization rates in Syria have decreased substantially since the start of the civil war, leaving a growing population of unvaccinated individuals, primarily children.
Israel, with a far more robust public health system than Syria and Somalia, has also seen evidence of the virus. Israel has an immunization rate of more than 95 percent and, like much of the developed world, uses the inactivated poliovirus form of the vaccine, which provides immunity for the vaccinated individual but is less effective than the oral vaccine at blocking transmission of the virus, leaving unvaccinated individuals at risk. The inactivated poliovirus vaccination does remove the risk of vaccine-derived infections, which remain rare with the oral form of the vaccine.
Polio and Vaccinations in Europe
Most of Europe also uses the inactivated poliovirus form of the vaccine. Infants typically begin the vaccination regimen within the first couple of months after birth. Overall, the average infant immunization rate for polio across Europe has fallen slightly since 2008, from 96 percent to 94 percent. While this drop is small and still above the threshold of 90 percent considered adequate, it indicates a trend in which a gradual accumulation of unvaccinated children (between 5 and 20 percent in some EU countries) increases the vulnerability of the population as a whole. Because herd immunity is not applicable in the case of the inactivated poliovirus vaccine, very high vaccination rates are required to ensure public protection. Polio immunization levels vary from country to country in the European region. The countries with the lowest infant immunization rates (below 90 percent) include Austria, Bosnia-Herzegovina, Georgia, Iceland and Ukraine. Countries below 95 percent include a few Western European nations — Denmark and Germany — along with Estonia, Latvia, Lithuania, Moldova, Montenegro and Romania.
Lower vaccination rates can be explained in part by the fact that polio no longer poses an immediate threat to the region. The European region was declared polio-free in 2002, and Western Europe has not seen an outbreak since 1992-1993, when the virus spread through an unvaccinated population cluster in a religious community in the Netherlands. An outbreak occurred in 2010 in Tajikistan, but it was confined to Central Asia. Thus, many countries in Europe have also become lax in terms of surveillance to track potential occurrences of the virus. This includes monitoring sewer systems for environmental evidence and identifying infections in which paralysis does not occur. The European Center for Disease Prevention and Control's risk assessment issued after the Syrian outbreak calls for heightened surveillance measures.
Immigrants and asylum seekers, particularly from Syria, have the greatest potential to introduce the poliovirus to the European community. Unvaccinated individuals in peripheral countries, which see the greatest influx of these populations, would correspondingly be at greater risk for infection.
The Geopolitical Effects of an Outbreak
Amid Europe's ongoing economic crisis, there has been concern regarding the Schengen zone — namely, allowing Romania and Bulgaria to join the treaty, which effectively removes border controls between participating nations. Health checks are not part of typical border checks, and the spread of a disease like polio, where not all carriers exhibit symptoms, is still possible even without Schengen participation. However, countries on Europe's periphery, such as Bulgaria, are major destinations for refugees trying to enter Europe, and the ability of these peripheral countries to control border inflows can come under greater scrutiny, particularly during disease outbreaks.
As part of efforts to halt the spread of disease, during outbreaks peripheral countries have used tighter border controls and even closures, including in 2009 with the swine flu outbreak. All four Schengen candidate countries have vaccination rates above 90 percent (Romania has the lowest rate at 92 percent). However, infections in other countries with lower immunization levels — Ukraine or Bosnia-Herzegovina, for example — amid an outbreak of a disease as psychologically frightening as polio could justify continued opposition to Romania and Bulgaria's Schengen membership and could fuel greater skepticism about broader European integration.
Alternatively, an occurrence of polio in an Eastern European country such as Ukraine, which is currently torn between Eastern and Western influences, could allow Western aid organizations to enter the country to prevent further spread of the disease. This could have an ancillary effect of increasing Western influence in the region.
No polio cases have been reported in Europe to date. Concerted efforts to increase immunization against polio across Europe would certainly decrease the risk of infection and could be used as a protective measure, but non-routine vaccinations are not recommended for the general population at this time. However, with the region on alert for a disease that has not been a real threat for more than a generation, the outbreak in the Middle East could shape political decisions in a region in flux. Fear of the disease could perpetuate both anti-immigration movements and opposition to the expansion of the Schengen zone.